How to Choose a Healthcare Marketing Agency in 2026: A Decision Framework
A seven-dimension decision framework for evaluating healthcare marketing agencies. Compliance, specialty, channel mix, measurement, case studies, team, and pricing.

Executive Summary
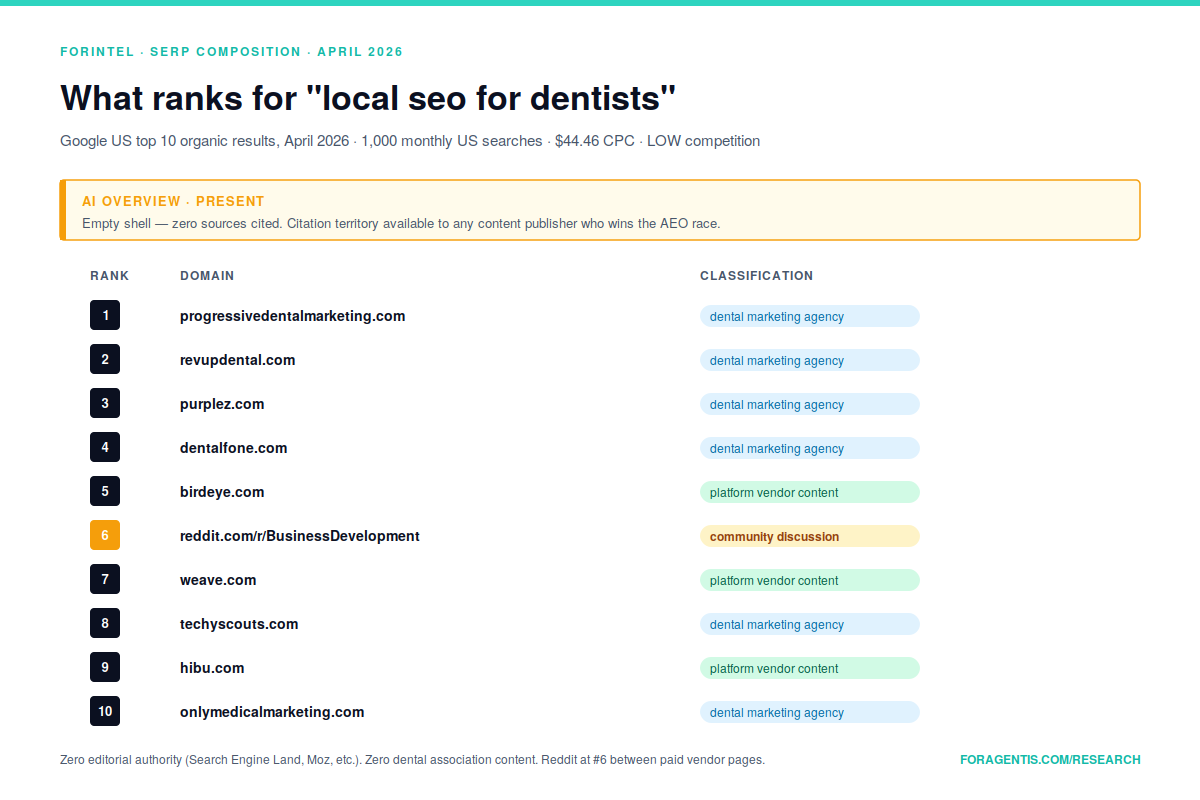
Healthcare marketing agency selection is one of the highest-stakes vendor decisions a medical practice, hospital system, or health tech company makes. Compliance exposure is category-specific, specialty expertise is not interchangeable, and the gap between competent and incompetent healthcare marketing work is measurable in patient acquisition economics and regulatory risk. The current market for healthcare marketing agencies carries meaningful commercial signal — best healthcare marketing agency registers 90 monthly US searches at a $21.28 CPC, one of the highest commercial-intent CPCs ForIntel research measured across 15 verticals — but the SERP is structured as a business-listing contest, not a content-knowledge contest.
This report is not a ranking of the best healthcare marketing agencies. That genre is well-populated, and the existing rankings are largely either directory-style listicles produced by ranking aggregators or promotional pages from agencies describing themselves. What is missing is a decision framework: a structured way for practice owners, hospital marketing directors, and health tech CMOs to evaluate agency candidates against the specific requirements of healthcare marketing work, so that the evaluation produces a decision rather than a shortlist of names.
The framework below organizes agency evaluation around seven dimensions: compliance expertise, specialty experience, channel mix, measurement philosophy, case study ownership, team structure, and pricing transparency. Each dimension is independently scorable. The combined scoring produces a 0-100 evaluation of any candidate agency, which can be applied consistently across a shortlist of 5-10 candidates.
For healthcare marketing buyers, the framework replaces the typical "we met with four agencies and picked the one we liked best" selection process with a defensible evaluation that surfaces the specific deficits and strengths of each candidate. For healthcare marketing agencies reading this report, the framework functions as a self-assessment scorecard — understanding how a sophisticated buyer will evaluate you is a prerequisite to being evaluated well.
Key Findings
Commercial demand signal is real and high-CPC.
Best healthcare marketing agencyregisters 90 monthly US searches with a $21.28 CPC.Healthcare digital marketing trendsregisters 40 monthly searches at $13.42 CPC.Healthcare marketing benchmarksregisters 10 monthly searches at $20.39 CPC — one of the highest CPCs in the healthcare content category (Google Ads keyword data, sample_count = 9 healthcare-specific phrases, April 2026).Volume is volatile but trending. The 6-month history for
best healthcare marketing agencyshows 110, 90, 30, 30, 20, 70 — a significant month-to-month range. Content investment against this keyword should assume the middle of the distribution, not the recent peak. Thehealthcare competitor analysishistory (30, 10, 20, 40, 40, 30) is more stable but at lower absolute volume.The healthcare agency SERP is a business-listing contest, not a content contest. The top 10 for
best healthcare marketing agencyconsists of eight agency homepages or directory-style listicles: Weinbach Group, Healthcare Success, Intrepy, Clarity QST, Onspire Health, Cardinal Digital Marketing, g-co.agency, and Practice Builders. Zero editorial publications rank. Zero horizontal SEO platforms rank.The audit SERP is thin and commercially contested.
Healthcare seo auditregistered 10 monthly searches with 3 of the last 6 months at zero. The keyword is below the threshold where sustained content investment is defensible as a primary ranking target. This does not invalidate healthcare audit content as part of a strategy, but it does mean the audit keyword should not be the flagship.Healthcare is OPEN on tool-vendor displacement. Across the Q5 counter-hypothesis test (sample_count = 22 healthcare SERP positions), zero horizontal SEO platforms (Semrush, Ahrefs, Moz, HubSpot, Profound, Writesonic, Conductor) rank in the top 10 for
healthcare seo benchmarks,healthcare marketing statistics 2026, orhealthcare digital marketing report. Healthcare content territory is contested by specialized healthcare agencies, vertical-specific research platforms (PulsePoint, Liine, Tebra), and trade publications.The healthcare guide SERP is contested but beatable. The top 10 for
healthcare seo guideis Healthcare Success, GetDearDoc, Siteimprove, Wheelhouse DMG, WordStream, GetHealthie, Sermo, SureOak, and Siteimprove again. No horizontal SEO platform ranks. The content quality is uneven — several ranking pages are framework-light and example-free. Genuinely rigorous healthcare SEO content has a plausible path to top-10 ranking, but the ranking anchor is Healthcare Success at position #1 with category authority built over more than a decade.Healthcare marketing agencies compete on specialty, not price. The top-ranked agency content consistently differentiates on specialty focus (dental, med spa, hospital systems, mental health, telehealth) rather than on pricing or general digital capability. This has implications for the evaluation framework: specialty expertise is the primary filter, not a tiebreaker.
Methodology
This report combines three data sources and one qualitative layer.
Search demand analysis. Monthly US search volume, competition index, cost-per-click, and 6-month historical volume data were pulled via Google Ads keyword endpoints for 15 healthcare-specific phrases across Pattern A (agency queries), Pattern B (benchmarks), and Pattern D (audit/competitor/guide). Sample_count = 15 healthcare keywords, April 2026.
Search intent classification. The same phrases were classified through DataForSEO Labs search_intent endpoint for primary intent label and confidence probability. Healthcare phrases showed commercial intent probabilities ranging from 0.69 (healthcare seo audit) to 0.95 (healthcare competitor analysis) to 0.58 (best healthcare marketing agency, which the classifier scored conservatively; the $21.28 CPC confirms commercial intent independently). Sample_count = 15.
SERP composition analysis. Top 10 organic results (US, desktop, English) were pulled for each phrase via serp/_/live/advanced. Each ranking position was classified by domain, title, URL, and result type. An additional SERP pull for neutral healthcare benchmark queries tested tool-vendor displacement (sample_count = 22 additional positions).
Independent review. Each finding was evaluated by an independent reviewer for disconfirming evidence, measurement artifacts, and interpretive alternatives. Counter-signals that survived review are reported alongside confirming findings in the analysis below.
All findings are cited to source. Effect-size estimates are descriptive rather than statistically inferential unless otherwise noted. Findings below the statistical-inference threshold are labeled as directional.
The 7 Dimensions of Healthcare Marketing Agency Evaluation
The framework below organizes agency evaluation across seven dimensions. Each dimension carries specific evaluation questions, expected answers, and common failure modes. The framework is designed to be applied consistently across a shortlist of 5-10 candidate agencies.
Dimension 1: Compliance Expertise
Healthcare marketing operates under regulatory constraints horizontal marketing does not face. HIPAA governs protected health information handling. FTC guidance governs claims about health outcomes. State regulations govern physician advertising, telehealth marketing, and direct-to-consumer pharmaceutical promotion. Google Ads' healthcare category restrictions shift with regulatory and policy updates.
Questions to ask a candidate agency:
- What is your process for HIPAA review of client-facing content?
- Do you have a Business Associate Agreement (BAA) template? Will you sign ours?
- How do you handle patient testimonials and case studies?
- What is your experience with FTC health claims review?
- What is your experience with Google Ads healthcare category compliance?
- Have any of your campaigns been flagged, paused, or removed by Google or Meta for healthcare compliance issues in the past 24 months? What was the resolution?
Expected answers from a competent agency: Clear documented processes for each area, named team members responsible for compliance review, examples of compliance-driven campaign adjustments with client approval, and willingness to sign BAAs without extensive negotiation. Agencies that treat compliance as an afterthought or as the client's responsibility produce campaigns that work until they don't.
Failure mode to flag. An agency that has never had a campaign flagged or paused by an ad platform for healthcare compliance is either (a) not running enough campaigns to test the edges, or (b) running only the most conservative content types. Neither is ideal. The right answer is "yes, we've had campaigns paused, and here's how we handled it."
Dimension 2: Specialty Experience
Healthcare is not one vertical; it is dozens. Dental practice marketing does not transfer cleanly to telehealth marketing. Med spa marketing does not transfer to hospital system marketing. Mental health marketing has specific regulatory and ethical constraints not shared by dermatology or cardiology. Agencies that claim competence across all healthcare specialties are usually competent in one or two and adequate at the rest.
Questions to ask:
- What healthcare specialties do you currently serve? (List named client categories, not generic capability claims.)
- How many current clients do you have in our specialty? (If zero, this is a specialty-onboarding engagement, not a specialty-competent one — priced and evaluated accordingly.)
- What patient acquisition economics benchmarks apply to our specialty? (If the agency cannot name cost-per-appointment-booked, cost-per-consultation-completed, or lifetime-value ranges for your specialty, they do not have the specialty data yet.)
- What specialty-specific compliance considerations apply? (A dental agency should know about informed consent photography release requirements. A mental health agency should know about crisis-intervention content guidelines.)
Expected answers. Specific named clients in your specialty (or explicit acknowledgment that your specialty is new to them, priced accordingly), concrete benchmark numbers, specialty-specific compliance awareness, and ideally case studies from your specialty available for reference.
Failure mode to flag. An agency that describes its healthcare capability in generic terms ("we work with all kinds of medical practices") is signalling that it does not differentiate its work by specialty. This is acceptable for general-purpose campaigns at scale but is a significant disadvantage for specialty-dependent work.
Dimension 3: Channel Mix
Healthcare marketing channels are not neutral. SEO, paid search, content marketing, local marketing, reputation management, and patient-nurture email all work differently in healthcare than in horizontal categories, and they work differently across healthcare sub-verticals.
Questions to ask:
- What channel mix do you recommend for a practice of our size and specialty, and why?
- How do you weight SEO against paid search for our patient acquisition goals?
- What is your approach to Google Business Profile optimization for multi-location healthcare practices?
- What is your approach to patient review velocity? How do you handle negative reviews?
- What is your experience with healthcare-specific local SEO (HCP directory submissions, specialty-specific citation profiles)?
Expected answers. A clear recommendation calibrated to your specialty and size, with reasoning tied to patient acquisition economics rather than channel-preference. Agencies that recommend the same channel mix to every client are either running a productized service (which is fine if priced and positioned as such) or are biased toward their own channel capabilities.
Failure mode to flag. An agency that recommends a disproportionate share of budget toward channels where they hold vendor partnerships or certifications (Google Premier Partner certification often correlates with Google Ads spend recommendations; HubSpot Partner status often correlates with inbound marketing recommendations) is optimizing the recommendation for their incentives, not yours.
Dimension 4: Measurement Philosophy
Measurement is the dimension where most healthcare marketing engagements quietly fail. Agencies track what they can measure cleanly — impressions, clicks, traffic, form submissions — and deprioritize what they cannot measure cleanly — patient acquisition cost, consultation-to-appointment conversion, lifetime value of acquired patients, specialty-specific quality signals.
Questions to ask:
- How do you measure patient acquisition cost (PAC)? What is our current PAC, and what do you project it will be 6 and 12 months into the engagement?
- How do you measure patient lifetime value (LTV)? Do you have access to our PMS/EHR revenue data, and if not, how do you estimate LTV?
- What is your approach to attribution for multi-touch patient acquisition journeys?
- How do you measure the contribution of brand awareness versus direct-response work?
- What measurement limitations do you operate under, and how do you communicate them to clients?
Expected answers. A clear measurement philosophy with named metrics, honest acknowledgment of measurement limitations (no agency can measure everything cleanly), and a willingness to structure reporting around the client's metrics of interest rather than the agency's standard metrics. Agencies that report only on vanity metrics (impressions, traffic, rankings) without connecting to patient acquisition economics are not aligned with your outcomes.
Failure mode to flag. An agency that claims to measure patient LTV without access to practice management system revenue data is either estimating LTV using industry benchmarks (which may or may not apply to your practice) or is not actually measuring LTV despite the claim.
Dimension 5: Case Study Ownership
Case studies are the agency industry's credibility currency. Healthcare case studies specifically carry compliance constraints — named patient stories require releases, named practice case studies require client approval, and numerical claims require context about time periods and methodology.
Questions to ask:
- Can you share 3-5 detailed case studies from practices similar to ours, with named clients or anonymized-with-context data?
- Will you provide a reference call with 2-3 current clients?
- What was the starting position of the featured case study clients (patient volume, digital maturity, existing agency relationships), and what was the end position?
- What methodology was used to attribute outcomes to your work versus other variables (seasonality, new provider hires, geographic market changes)?
- What percentage of case study clients remain clients today?
Expected answers. Detailed case studies with specific numerical claims and context, willingness to provide reference calls, and honest context about the client's starting position and other variables that contributed to outcomes. The retention rate question is diagnostic — an agency whose case study clients have largely churned is either producing good short-term results that do not sustain or is cherry-picking historically successful clients.
Failure mode to flag. An agency that presents anonymized case studies only, refuses reference calls, or cannot provide retention data is either in a confidentiality-heavy portfolio (which is defensible for large health systems) or is protecting a thinner track record than their pitch implies.
Dimension 6: Team Structure
Team structure determines whether the senior people in the pitch meeting are the people actually working on your account. Healthcare marketing work is sufficiently specialty-dependent that this question is not a formality.
Questions to ask:
- Who specifically will be working on our account, and what is each person's specialty experience?
- What is the ratio of junior to senior time on our account, and how does that ratio change over the engagement?
- Who is our account's day-to-day contact, and what is our escalation path?
- What is the agency's approach to account team continuity? What happens if our primary contact leaves the agency?
- Can we meet the proposed account team before signing?
Expected answers. Named people with specialty-relevant experience, honest senior/junior ratios, clear escalation paths, and willingness to introduce the account team before signing. Agencies that pitch with senior leaders but staff with junior teams are producing junior work at senior pricing.
Failure mode to flag. An agency that cannot name the specific team members who will work on your account is either a pooled-resource model (acceptable for some productized services, unacceptable for specialty work) or is selecting the team after the contract signs based on who has availability.
Dimension 7: Pricing Transparency
Healthcare marketing agency pricing is notoriously opaque. Retainer structures, performance-based structures, hybrid structures, and commission-based structures all carry different incentive alignments.
Questions to ask:
- What is your pricing structure? Is it retainer-based, performance-based, hybrid, or commission-based?
- What is included in the base engagement, and what triggers additional billing?
- What is your minimum engagement commitment?
- How is paid media spend handled — pass-through, marked-up, or agency-managed with transparency?
- What is the typical first-year engagement cost for a practice of our size and specialty?
- What is your approach to scope changes during an engagement?
Expected answers. Clear pricing structure with explicit delineation of scope, transparent handling of paid media spend, honest discussion of minimum commitments, and willingness to provide typical-engagement cost ranges. Agencies that refuse to discuss pricing before multiple exploratory meetings are either running a high-touch sales process that may not deliver proportional value or are pricing each engagement opportunistically based on perceived client budget.
Failure mode to flag. An agency that marks up paid media spend by 10%+ without disclosing the markup as a commission is operating under a conflict of interest — the agency's revenue scales with recommended media spend, which biases channel-mix recommendations.
What the Data Shows
Finding 1: The Agency SERP Is Business-Listing Territory, Not Content Territory
The top 10 for best healthcare marketing agency (April 2026) consists of eight agency homepages or directory-style listicles: Weinbach Group (#1, a listicle), Healthcare Success (#2, agency homepage), Intrepy (#3, agency service page), Clarity QST (#4, listicle), Onspire Health (#5, agency), Cardinal Digital Marketing (#6, agency), g-co.agency (#7, listicle), and Practice Builders (#8, agency). There is no AI Overview on this SERP.
This composition differs from the ecommerce and SaaS SERPs analyzed in companion reports. The horizontal SEO platforms are absent (as they are across healthcare). But so are editorial publications, trade magazines, and research firms. The best healthcare marketing agency SERP is a contest between agencies selling themselves and directories selling their aggregation. This is significant for content strategy: a framework piece that sits above a listicle (which this report attempts) occupies uncontested content territory, but it will not easily outrank Weinbach's listicle format on the specific keyword — the keyword is structurally biased toward listicle format in Google's current ranking logic.
Implication. The realistic goal for a framework piece like this report is to rank for adjacent keywords (how to choose a healthcare marketing agency, healthcare marketing agency evaluation, healthcare marketing agency questions to ask) while the listicles continue to occupy the head-term SERP. The two content types serve different buyer moments and should not be forced into direct competition.
Counter-signal. Adjacent keywords may have even thinner volume than the head term. Healthcare marketing agency evaluation returned null volume in this sample keyword measurement. Ranking well for zero-volume keywords does not produce traffic.
Finding 2: CPC Signals Are the Strongest Commercial Indicator for Healthcare
Where search volume signal is thin, CPC signal is strong. Best healthcare marketing agency carries a $21.28 CPC. Healthcare marketing benchmarks carries a $20.39 CPC. Healthcare digital marketing trends carries a $13.42 CPC. In a context where the intent classifier scored best healthcare marketing agency at only 0.58 commercial probability (conservative), the CPC data is the stronger commercial indicator.
CPCs in this range exist because paid advertisers are actively bidding. The implication is that the healthcare agency market has real commercial activity and real buying signal, but the buying signal is distributed across a small number of terms rather than aggregated into high-volume head terms. Healthcare marketing buyers are active, specific, and willing to pay; they are not searching in large aggregated volumes.
Finding 3: Healthcare Vertical Content Is Open on Tool-Vendor Displacement
The Q5 counter-hypothesis test (sample_count = 110 positions across 11 vertical benchmark SERPs) classified healthcare as OPEN — zero horizontal SEO platforms in the top 10 for healthcare seo benchmarks, healthcare marketing statistics 2026, or healthcare digital marketing report. The content is contested by specialized healthcare agencies (WebFX, Promodo, Cardinal Digital Marketing), vertical-specific research platforms (PulsePoint, Liine, Tebra, APQC), and trade publications (Becker's Hospital Review, SHSMD).
This pattern repeats across ForIntel research's vertical coverage. For healthcare specifically, the implication is that a mid-authority domain producing genuinely vertical-specific content with proprietary data has a plausible path to top-10 ranking on benchmark and statistics queries. The existing rankers are beatable on research quality rather than on domain authority alone.
Counter-signal. The healthcare benchmark keywords returned null or very thin search volume (healthcare marketing benchmarks at 10/mo, most others null). The market signal from these keywords comes from CPC and SERP competition, not from search volume. Investing heavily in benchmark content for healthcare is defensible as a credibility asset but should not be expected to drive traffic at scale.
Finding 4: The Healthcare Guide SERP Is Contested by Vertical Specialists, Not Horizontal Platforms
The top 10 for healthcare seo guide is Healthcare Success (#1), GetDearDoc (#2), Siteimprove (#3), Wheelhouse DMG (#4), WordStream (#5), GetHealthie (#6), Sermo (#7), SureOak (#8), and Siteimprove again at #9 with a different article. All are healthcare-specialized or horizontal content publishers. No horizontal SEO platform ranks.
Healthcare Success at #1 carries meaningful category authority — they have published healthcare SEO content for more than a decade and their domain authority on the healthcare-agency sub-vertical is defensible. Positions 2-9 are contested by mid-authority domains whose content quality is uneven. Several ranking pages in this SERP are framework-light, example-free, or cross-vertical SEO content with "for healthcare" appended rather than genuinely healthcare-specific.
Implication. Rigorously produced, specifically-healthcare SEO content from a mid-authority domain has a plausible path to top-10 ranking, but displacing Healthcare Success at #1 requires a decade-plus content investment, not a quarterly campaign.
Finding 5: AI Overview Is Absent on Most Healthcare Commercial Queries
Among the healthcare SERPs analyzed, AI Overview presence is uneven. Best healthcare marketing agency shows an AI Overview shell with empty references. Top healthcare seo agencies shows the same empty-shell pattern. Healthcare competitor analysis has a featured snippet (Invoca) but no AI Overview. Healthcare digital marketing trends has a featured snippet (g-co.agency) and no AI Overview.
The empty-shell pattern on commercial healthcare queries is consistent with the pattern observed in ecommerce and SaaS benchmark queries — Google recognizes these as synthesis-eligible queries but does not find content authoritative enough to quote, or actively withholds sources for reasons internal to Google's answer-layer logic. The analytical implication is that AI Overview optimization for healthcare agency and commercial queries should be deprioritized in favor of AI Overview optimization on patient-facing educational queries (where the buying moment is different and AI Overviews are more active).
Implications for Healthcare Practice Owners and Marketing Directors
For healthcare practice owners, hospital marketing directors, and health tech CMOs running agency evaluations, three practical implications follow from the framework and findings.
First, evaluate candidates against the seven dimensions before sitting through four pitch meetings. A structured evaluation surfaces the specific deficits of each candidate before those deficits become operational problems. The sales polish of a pitch meeting is not diagnostic of the working relationship.
Second, prioritize specialty experience as the first filter. An agency with deep specialty expertise is structurally more valuable than an agency with deep cross-healthcare expertise, even if the specialty-focused agency appears smaller or less sophisticated in its pitch. Generic healthcare marketing capability is a commodity; specialty expertise is not.
Third, require case study retention data. Agencies that cannot or will not provide client retention rates are hiding information that is material to your decision. A 60% one-year retention rate signals short-term results that do not sustain. A 90% two-year retention rate signals genuine competency. The data is not hard to report; its absence is diagnostic.
Implications for Healthcare Marketing Agencies
For healthcare marketing agencies reading this report, the seven-dimension framework functions as a self-assessment. An agency that scores itself honestly against the framework surfaces its own deficits — compliance gaps, over-generalized specialty claims, measurement blind spots, case study retention problems, opaque pricing structures — before a sophisticated client surfaces them in evaluation.
Agencies that want to move up the evaluation curve with buyers using structured frameworks like this one have three durable paths: specialty concentration (becoming the category leader in one healthcare sub-vertical), measurement depth (investing in patient acquisition economics infrastructure that lets you report LTV and PAC accurately), and case study discipline (producing detailed, named, retention-tracked case studies rather than anonymized one-offs).
For agencies that want to strengthen their competitive positioning with proprietary research, ForIntel Vertical Intelligence Reports produce healthcare vertical and sub-vertical analyses calibrated to the specialties each agency serves.
Limitations
This report carries five meaningful limitations.
First, all search volume, SERP, and intent data is US-only. Healthcare marketing markets outside the US operate under different regulatory regimes (PHIPA in Canada, NHS constraints in the UK) and different patient acquisition economics. Generalization across geographies is not supported by this data.
Second, the seven-dimension framework is diagnostic rather than prescriptive. It surfaces deficits in candidate agencies but does not specify the relative weight each dimension should carry for a specific buyer. A rural independent practice may weight pricing transparency and team structure heavily; an urban multi-specialty hospital system may weight compliance expertise and specialty experience more heavily. The framework is starting point, not a formula.
Third, healthcare vertical search volumes are particularly thin. Most of the 15 tested healthcare keywords returned null or single-digit monthly volume. Commercial signal in this vertical comes from CPC data and SERP competitive activity, not from search volume aggregation. Content investment against healthcare agency-related keywords should be justified on credibility and authority-building, not on direct traffic projections.
Fourth, AI Overview behavior is in active flux. AI Overview presence on healthcare queries may resolve (empty shells populating with sources) or deteriorate (populated AIOs losing sources) within 6-12 months. Quarterly re-measurement is required.
Fifth, the framework does not evaluate agency creative quality, which is genuinely important for healthcare marketing and is genuinely difficult to measure through structured evaluation. Creative quality evaluation requires reviewing work samples, which is a qualitative exercise the framework does not replace.
These limitations do not invalidate the framework; they bound the claims the framework supports.
Future Research
Three natural extensions of this report are worth noting.
The first is specialty-specific framework adaptations. Dental practice marketing, med spa marketing, hospital system marketing, mental health marketing, and telehealth marketing each carry specific regulatory, operational, and economic constraints that may warrant dimension re-weighting or dimension additions.
The second is longitudinal measurement of agency-evaluation outcomes. A 12-month post-evaluation study of practices that applied a structured evaluation framework against practices that did not would produce data on whether structured evaluation improves agency-selection outcomes.
The third is a comparable framework for adjacent professional services (dental practice management consulting, healthcare technology vendor selection, clinical research organization evaluation) to test whether the seven-dimension framework generalizes across healthcare-adjacent professional service buying decisions.
Download the Companion Evaluation Template
The 2026 Healthcare Marketing Agency Evaluation Template is a 35-step scoring rubric built around the seven-dimension framework with a 0-100 evaluation output. Two versions are available: one for practice owners and marketing directors evaluating candidate agencies, and one for agencies using the framework as a self-assessment. Enter your email to receive both PDFs.
Download the Buyer Version → Download the Agency Self-Assessment Version →
Get Your Own Vertical Intelligence Report
This report profiles one vertical. The ForIntel methodology is designed to produce comparable analyses across any B2B or B2C vertical where search demand, content competition, backlink patterns, and AI citation behavior need to be understood before committing resources.
A custom ForIntel Vertical Intelligence Report includes: search demand analysis across vertical-specific keyword sets; SERP competitive landscape with backlink profiles and content patterns; AI Overview citation mapping across major LLMs; content-gap identification based on what top rankers are not serving; buyer archetype profile grounded in search language and community register; and a prioritized distribution plan calibrated to the vertical's specific channels.
Request a Custom Report → Schedule a Consultation →
About ForIntel
ForIntel is the intelligence research layer produced by Foragentis, a Sacramento-based AI research and product company. Foragentis operates ForaPost, an AI-powered social media management platform serving small and medium businesses across more than fifty verticals and eight major platforms, and ForIntel, the intelligence system that produced this report.
The methodology combines programmatic data collection from search, SERP, backlink, and LLM-citation data with independent verification and human-in-the-loop inspection. Every finding in this report is traceable to its underlying data, and claims that did not meet statistical or sample-size thresholds are labeled as directional rather than validated.
For healthcare practices managing their own social media presence across patient-facing channels, ForaPost's 8-platform publishing and approval workflow is available at Pro ($29/month) and Panorama ($59/month) tiers, with a 14-day free trial. HIPAA-aware content production workflows are documented in the ForaPost healthcare guide series.
Try ForaPost Free for 14 Days →
Contact forintel@foragentis.com or visit https://foragentis.com/forintel#order to scope a custom report.
Frequently Asked Questions
How do you evaluate a healthcare marketing agency?
Score candidates across seven dimensions: compliance expertise, specialty experience, channel mix, measurement philosophy, case study ownership, team structure, and pricing transparency. Apply the same scoring to every shortlisted agency and compare dimension-level scores to identify specific strengths and deficits.
What questions should I ask a healthcare marketing agency?
Ask about HIPAA review processes, willingness to sign Business Associate Agreements, FTC health-claims review experience, campaigns flagged by ad platforms for healthcare compliance, and named team members with documented specialty experience in your specialty.
How much does a healthcare marketing agency cost in 2026?
Pricing varies by structure (retainer, performance-based, hybrid, commission) and specialty. Ask for typical first-year engagement cost for a practice of your size and specialty before committing.
What is a Business Associate Agreement and do I need one?
A Business Associate Agreement (BAA) is a HIPAA-required contract when a marketing agency has access to protected health information. Every healthcare marketing agency engagement that touches patient data requires one.
Is SEO or paid search more effective for healthcare practices?
Neither is universally correct. The right channel mix depends on specialty, patient acquisition economics, and local competitive conditions. Agencies that recommend the same channel mix to every client are running a productized service or are biased toward their own channel capabilities.
© 2026 Foragentis. This report may be cited with attribution. Redistribution requires permission.
Related ForIntel reports
ForIntel produces the kind of research above on commission. These SKUs answer the questions this piece raises — directly, on a fixed timeline, with sources cited.